States Are Missing the Most Important Use of RHTP Funding.
And Rural Hospitals Will Pay for It.
Congress authorized mechanical equipment replacement as an eligible use of $50 billion in rural healthcare funding. Most states are spending it on telehealth and technology instead. Here is why that is the wrong call and what rural hospitals should do about it.
The Rural Health Transformation Program is the largest federal investment in rural healthcare in decades: $50 billion distributed to all 50 states from 2026 through 2030. Every state received an award. The federal framework explicitly authorizes equipment upgrades and mechanical infrastructure replacement as an eligible use of funds. The stated rationale in the federal NOFO is straightforward: ensuring operating costs are commensurate with patient volume.
Most states are not spending it that way.
A review of state RHTP applications reveals a consistent pattern: workforce development, telehealth expansion, AI tools, behavioral health, and EHR modernization dominate state spending plans. Facility infrastructure and mechanical equipment replacement, the federal use category most directly tied to rural hospital financial survival, has been largely overlooked.
That is a significant mistake. And rural hospitals have a narrow window to change it.
WHAT STATES ARE ACTUALLY SPENDING RHTP MONEY ON
All 50 states structured their applications around five strategic goals established by CMS: Make Rural America Healthy Again, Sustainable Access, Workforce Development, Innovative Care, and Technology Innovation. In practice, state plans have converged heavily on a few dominant themes:
• Telehealth infrastructure and remote patient monitoring
• Electronic health record modernization and interoperability
• Clinical workforce pipelines, residency programs, and retention incentives
• Behavioral health expansion and community-based care models
• AI-enabled clinical tools and rural technology catalyst funds
These are not bad investments. But they share a common characteristic: they are visible, politically compelling, and easy to frame as transformation. A drone pharmacy pilot or an AI scribe program makes for a better press release than replacing a 25-year-old chiller.
Facility infrastructure and mechanical equipment replacement, explicitly authorized under capital expenditure Category J of the federal NOFO, has been treated as a secondary priority in most state plans, if it appears at all.
“Investing in existing rural healthcare facility buildings and infrastructure, including minor building alterations or renovations and equipment upgrades to ensure long-term overhead and upkeep costs are commensurate with patient volume.”
That language is not ambiguous. Congress and CMS both anticipated that rural hospitals would use this funding to address aging mechanical infrastructure. Most states have not made it a priority in their distribution criteria.
WHY THIS IS THE WRONG CALL
The financial case for prioritizing mechanical infrastructure over technology investments is direct and compelling. It starts with understanding what actually closes rural hospitals.
Rural hospitals do not close because they lack AI scribes. They close because their operating costs exceed their revenue, and they cannot access the capital to address the infrastructure driving those costs. The single largest controllable component of a rural hospital's operating budget, after labor, is energy. And energy costs are overwhelmingly determined by the age and condition of mechanical systems: HVAC, boilers, chillers, building automation, and controls.
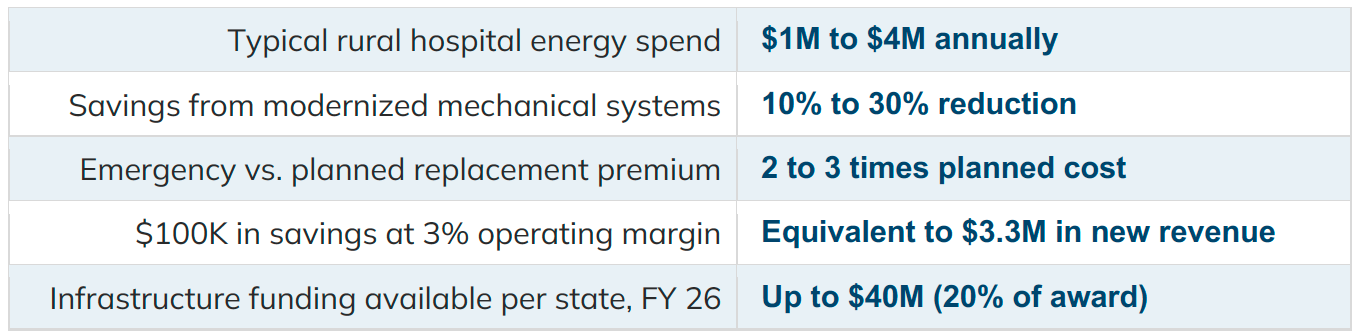
A rural hospital running a 25-year-old HVAC system is not just paying for deferred maintenance risk. It is paying an energy premium every single month: an invisible tax on every dollar of margin. When that system fails, the hospital faces emergency replacement at two to three times the cost of planned replacement, on a timeline that does not align with budget cycles.
The deferred maintenance backlog in rural healthcare is not a facilities problem. It is a financial solvency problem. Consider what the numbers look like:
Now compare this to the return profile of a telehealth platform or an AI tool. Both may improve access and care quality over time. Neither immediately reduces the operating cost structure of a facility already at the margins. Neither prevents the failure of a boiler during a January deep freeze.
Technology investments funded by RHTP will generate ongoing costs the moment the grant ends: software subscriptions, maintenance contracts, staff training, platform fees. Mechanical infrastructure replacements generate ongoing savings the moment they are completed. The financial logic is not close.
THE SUSTAINABILITY PROBLEM STATES ARE CREATING
RHTP is a five-year program. CMS has been explicit: this is not a permanent funding stream. States are required to demonstrate how their investments will produce sustainable outcomes after 2030.
Technology-heavy state plans have a structural sustainability problem. When the RHTP ends, the telehealth platform still needs to be licensed. The AI tool still requires a vendor contract. The new EHR integrations still need ongoing support. The rural hospital is left with a higher cost base and the same aging mechanical systems it had before.
Mechanical infrastructure replacement is self-funding in a way that technology investments are not. A replaced HVAC system does not send a monthly invoice. It generates energy savings from day one, permanently reduces operating exposure, and eliminates the emergency replacement risk that hangs over every aging system. The hospital is financially stronger after the investment than before it; independent of any ongoing grant relationship.
RHTP was designed to transform rural health. Replacing a failing boiler transforms the financial viability of the hospital that serves the community. That is the definition of transformation.
WHAT THE FEDERAL FRAMEWORK ACTUALLY ALLOWS
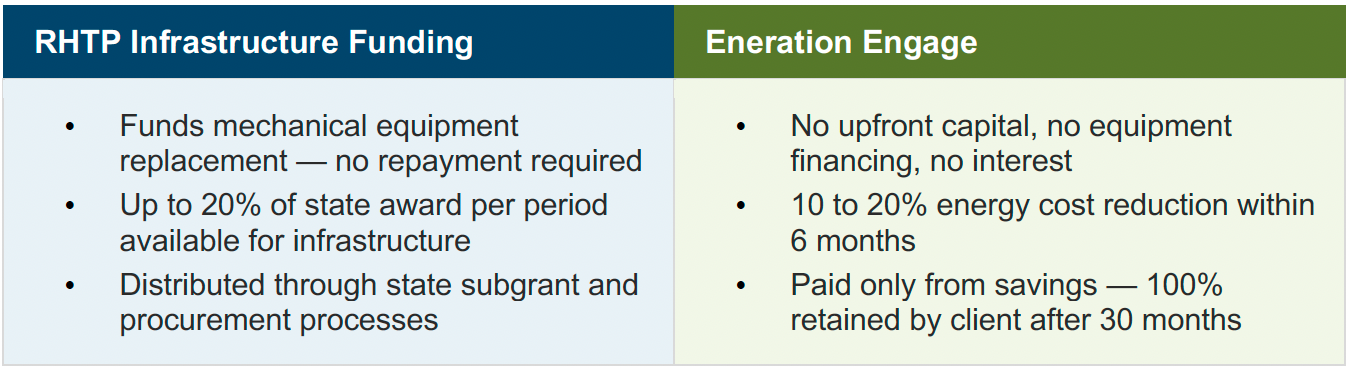
The NOFO is clear. Infrastructure and capital expenditures, including equipment upgrades, are an allowable use, capped at 20% of each state's award per budget period. At the average $200 million state award, that is up to $40 million annually for facility infrastructure, including mechanical systems.
What is not allowed is new construction. But replacement of existing equipment is explicitly permitted and that covers the most pressing deferred maintenance items rural hospitals carry: HVAC systems, boilers, chillers, building automation systems, and lighting infrastructure. The federal authorization is not ambiguous. The gap is at the state level, where distribution criteria have been designed around technology and workforce priorities rather than the infrastructure category Congress authorized.
Rural hospitals have both the standing and the strategic interest to advocate for their state to include mechanical infrastructure replacement in RHTP subgrant criteria. States that have not finalized their distribution processes, and most have not, still have the opportunity to correct course.
PAIRING RHTP WITH A SHARED-SAVINGS ENGAGEMENT
For rural hospitals that secure RHTP infrastructure funding, the question becomes: how do you ensure the replacement delivers the financial return it should?
Replacing aging mechanical equipment with modern, efficient systems generates measurable energy savings, but only if the implementation is managed with energy performance as the explicit goal, not just equipment swapping. That is the difference between a facilities contractor installing a new boiler and an energy management partner building a performance baseline, implementing ECMs, and measuring savings against it.
Eneration's Engage model is designed precisely for this. We establish a baseline, implement energy conservation measures, and are paid only from the savings we generate. RHTP funds the capital replacement. Eneration captures and sustains the energy performance gains. The hospital ends up with modernized infrastructure, validated energy savings, and no ongoing cost to either program.
WHAT THE RESULTS LOOK LIKE
Eneration was built by the team that created Gundersen Health System's energy independence program: the first health system in the United States to produce more energy than it consumed. That program generates $6M in annual savings and reduced emissions by 80%. The same fundamentals, applied at smaller rural facilities:
At a 3% operating margin, $100,000 in annual energy savings is the financial equivalent of $3.3 million in new revenue.
WHAT RURAL HOSPITALS SHOULD DO RIGHT NOW
Most states have not finalized their RHTP subgrant and procurement criteria. The window to influence those criteria, and to position your facility to access infrastructure funding, is open right now, but it will not stay open long.
1. Contact your state health department or rural health association today.
Ask specifically whether mechanical equipment replacement and energy infrastructure are included in your state's RHTP subgrant criteria. If they are not, advocate for their inclusion. States are still refining their distribution processes.
2. Inventory your deferred mechanical systems.
HVAC, boilers, chillers, building automation, and controls and document their age, failure risk, and current energy and maintenance costs. This is the application narrative you will need.
3. Request a no-cost Energy Performance Analysis from Eneration.
Establish your energy baseline and quantify the savings potential of modernized equipment. This analysis strengthens any RHTP application and is the foundation of a shared-savings engagement.
4. Structure the ask as an integrated initiative.
RHTP funds the capital replacement, Eneration captures and sustains the energy savings. No capital from the hospital. No ongoing cost. Immediate and permanent operating improvement.
Eneration assumes the performance risk. We are paid from savings generated, not before. If the savings are not there, we do not get paid.
About Eneration
Healthcare-exclusive energy management built by the team that created Gundersen Health System's energy independence program — the first health system in the United States to produce more energy than it consumed. We work with rural hospitals, critical access hospitals, and regional health systems across the country to reduce energy costs 10 to 30% in six months with no upfront capital, no equipment financing, and no long-term contracts. We are paid from the savings we generate.